When a #Plandemic Becomes a #Shamdemic
Guest Post
Obfuscated, fabricated death counts
There is evidence that the US Centers for Disease Control (CDC), as well as the governments of Italy and China – and thus likely many other governments – are or have been essentially cooking their COVID books to fake an epidemic by falsely counting deaths from other conditions as COVID or “COVID-associated” deaths. The Chinese in particular appear to have faked the virus, as they have neither isolated, photographed or biochemically and structurally characterized it, nor have they or world scientists subjected it to peer review. A UC Davis “genomic data scientist” computer-modeled the presumed new virus’s structure.
In reality this may have more to do with the existential question of the virus, very interesting material about which is still forthcoming. Suffice it to say preliminarily: One cannot culture and grow a virus in a petri dish like a bacterium can be grown. This is well known to scientists. Culturing a virus requires the addition of other cells, which are then, if there are “cytopathic” – in reality we’d say this is cytotoxic, not cytopathic – changes to the cell, presumed to have been caused by what is presumed to be a virus. From Wikipedia:
Viral culture is a laboratory test in which samples are placed with a cell type that the virus being tested for is able to infect. If the cells show changes, known as cytopathic effects, then the culture is positive.[1]
What the Chinese (along with some Australian scientists) have done is sequence a nucleic acid in some material they suspected but did not confirm of causing antibiotic-resistant pneumonia, which is found here. Why should they have conclusively assumed a virus was to blame? Antibiotic-resistant bacteria is known to be a top global health problem, cited as such by the World Health Organization (WHO) and in many scientific papers. And pneumonia due to air pollution is well known to be an actual epidemic in China, especially Wuhan, which saw vigorous air pollution protests in the summer of 2019. Still the Chinese CDC recorded the cause as “unknown origin”.
Today in fact CNN reports that the Chinese Ministry of Education’s science and technology department in March issued a directive mandating that “academic papers about tracing the origin of the virus must be strictly and tightly managed.”
China has imposed restrictions on the publication of academic research on the origins of the novel coronavirus, according to a central government directive and online notices published by two Chinese universities, that have since been removed from the web.
Earlier in the alleged global pandemic crisis, it was found that a change in counting methods created a soaring death toll in China. Hubei province, which accounted for roughly 80% of Chinese cases, saw its greatest one-day jump – a familiar pattern also seen in other countries – when officials decided to use “lung imaging” (i.e., a CT scan) instead of PCR (polymerase chain reaction) tests to “clinically diagnose” patients. “If lung images show pneumonia, patients who are already marked as suspected cases are confirmed as infected without the need for a positive RT-PCR test,” reported Channel News Asia in an article now removed from the Internet. “Suspected” cases included anyone who had traveled to Wuhan or surrounding areas, or who had contact with confirmed COVID cases or Wuhan visitors, and had symptoms such as a fever or low white blood cell count.
Of course, the PCR tests used in China (and everywhere else, for many purposes) are widely known to be neither precise nor reliable either: “Patients test positively if the genetic sequence of their blood or respiratory tract sample has a “high degree” of similarity with that of the virus.” Reports of 80% false positives in “asymptomatic individuals” and recovered patients were reported from China at that time. The former was retracted however. The creator of the PCR test, Kary Mullis, who died perhaps not uncoincidentally in August 2019, long ago acknowledged it could not work for the purposes for which it is routinely used in medical science.
These facts, taken together with China’s epic lockdown move, its separation of suspected infected family members, its passage of mandatory vaccination laws and the 2019 ramping-up of vaccine production, as well as the participation of Chinese CDC official George Gao in the Event 201 exercise and the “live exercise” (he’s been reported to have been in tears over the pandemic), seem to present sufficient cause for skepticism as to everything the Chinese have put out.
As for Italy, Angelo Borelli, its chief of “Civil Protection”, has stated that Italy “count[s] all the deceased. We do not differentiate between corona infected people who have died and those who have died because of the CV.” A March 20 report by its ISS (National Institute of Health) reported that 12% of deaths “have shown a direct causality from coronavirus, while 88 percent of patients who have died have at least one pre-morbidity – many had two or three,” according to Professor Walter Ricciardi, scientific adviser to the Italian government.
From the UK Telegraph:
The Italian health system counts not only people who died directly from coronavirus but also who died with coronavirus, regardless of whether or not they were suffering from one or more serious diseases when they contracted it.
“The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus,” said Prof Walter Ricciardi.
A much-read Bloomberg report noted that three days earlier, March 17, the Italian health authority reported that 99% of COVID-19 cases in Italy “had other illnesses”.
Northern Italy is also widely known to have bad air quality.
Similarly, in the US, the Centers for Disease Control (CDC) issued guidance to health care professionals, as is widely reported, as of March 24: “COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death.” The new diagnostic code was in actuality issued to the CDC by the World Health Organization (WHO) “for clinical or epidemiological diagnosis of COVID-19 where a laboratory confirmation is inconclusive or not available.” This occurred before the US epicenter of the alleged virus outbreak, New York City and New Jersey, reached their peak cases reports and deaths.
In its April 2020 guidance, the CDC, as the New York Times has it: “instructed officials to report deaths where the patient has tested positive or, in an absence of testing, ‘if the circumstances are compelling within a reasonable degree of certainty.’”
Trump’s COVID Task Force member Dr. Deborah Birx confirmed in the Coronavirus Task Force press conference of April 7 that the CDC is taking a “liberal approach to mortality”. She said in response to a question about coronavirus “deaths being misreported”:
“I think the reporting here has been pretty straightforward over the last five to six weeks…. There are other countries that if you had a preexisting condition and let’s say the virus caused you to go to the ICU and then have a heart or kidney problem, some countries are reporting that as a heart issue or a kidney issue and not a COVOD-19 death. Right now we’re still reporting it. And we’ll, I mean the great thing about having forms that come in and a form that has the ability to market [our emphasis] as COVID-19 infection, the intent is right now if those, if someone dies with COVID-19, we are counting that as a COVID-19 death.”
One will note that Birx directly contradicts what the Italian government has maintained all along, which is that Italy has also counted other morbidities as “comorbidities” of COVID-19 deaths. We suspect all countries have done this, but this will also have to be further proven.
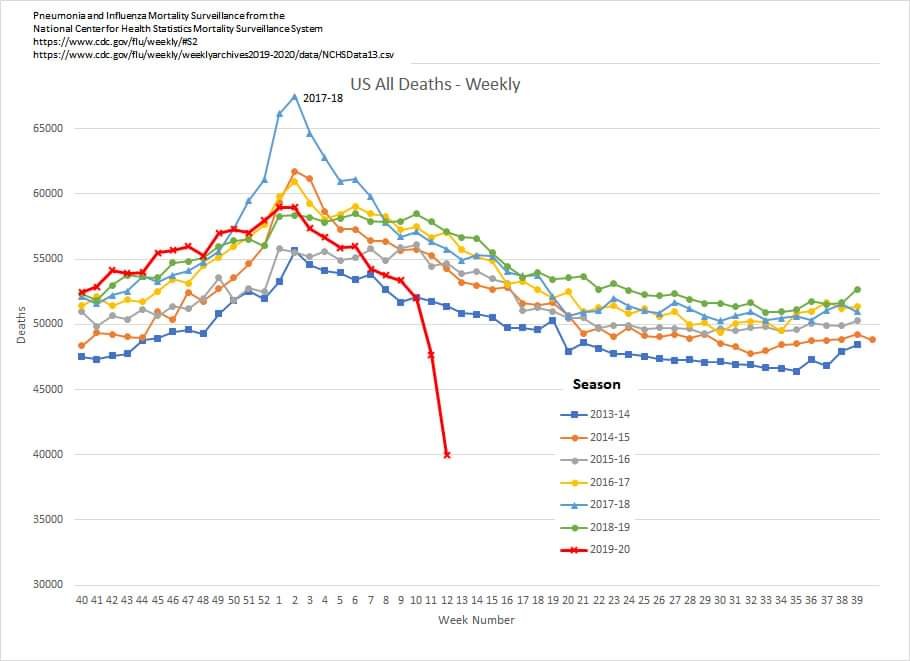
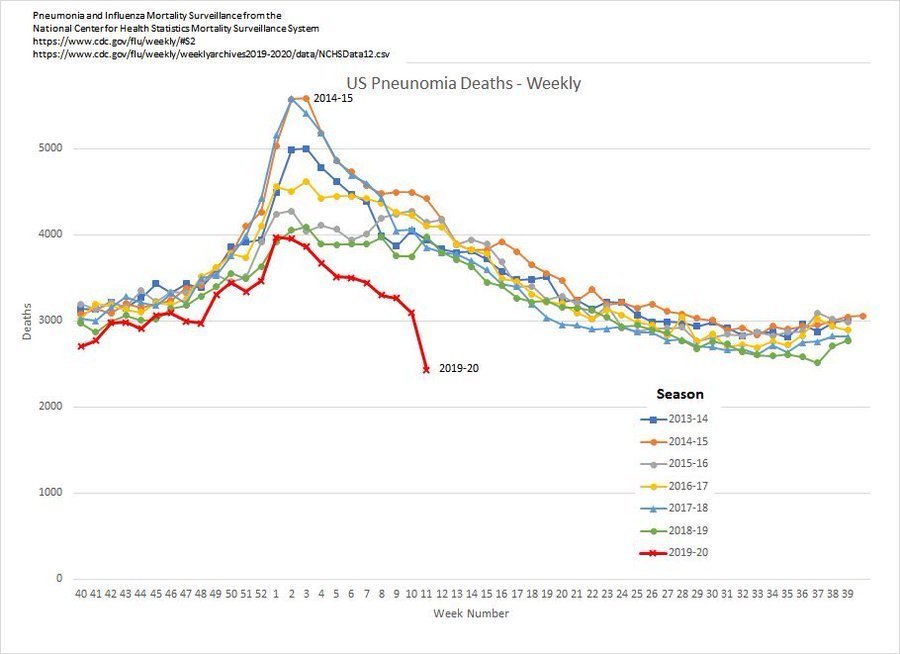
CDC’s statistics show that pneumonia and other deaths plummeted this year relative to prior years’ rates for the end of March and early April, as COVID rates began to rise around the US.
And yet, deaths from COVID-19 with “comorbidities” are the overwhelming majority not only in Italy but also in the US. An early mid-March CNN report of the US’s first “coronavirus” victims showed a majority of elders with pre-existing conditions – but no names reported by CNN. One New Jersey man with “diabetes, hypertension, atrial fibrillation, gastrointestinal bleeding and emphysema” and who had had two heart attacks was listed as a COVID-19 death.
More recently USA Today reported that 86% of New York COVID-19 decedents had “underlying illnesses”, while The Gateway Pundit cited official New York City statistics as of April 2 showing that only 1.29% of New Yorkers alleged to have died from COVID-19 had no “pre-existing conditions”. As the Pundit noted, these statistics were in line with the picture from China and Italy, with 99% having pre-existing conditions as of the date reported.
And, it should be noted that the 61-year-old Chinese man who was reported as the first “Wuhan coronavirus” death in December 2019 also suffered from “abdominal tumors and chronic liver disease”, according to a January 11 Science Magazine report.
China now reports a lower comorbidity rate of 25% based on an analysis of 37% of hospitals in China. Another more recent study, however, shows 74.4% of decedents had one or more preexisting condition, of which 50% was hypertension. But this is data derived from a study of only nine days in January and appears to be directed at the idea that the alleged virus has an ACE2 (angiotensin-converting enzyme II) receptor, which plays a critical role in cardiac physiology among other bodily processes. The new report notes: “clinical studies are also needed to confirm whether angiotensin-converting enzyme inhibitors and angiotensin receptor blockers could be beneficial for patients with COVID-19”. Several articles have appeared suggesting these types of drugs would or already benefit COVID-19 patients.
But, given this issue of statistical reporting (among other issues of testing and identification of the alleged pathogen itself), it is an absolutely legitimate question as to who, if anyone, has actually died of COVID-19. Since much evidence indicates the virus does not actually exist, we’d answer this in the negative, but this is yet to be further proven in later work. The statistical picture shown here already already suggests circumstantial evidence that the virus does not exist as such.
Data indicating that more males than females have officially died of COVID-19 globally also suggest that it is other morbidities and not “comorbidities” that have driven the alleged deaths, which are generally greater in men than women globally.
Official explanations from the CDC state that comorbidities indicate a “higher risk” for “severe illness from COVID-19”.
New York City hospitalization and death figures of 29,335 and 6,182 respectively as of April 13 continue to defy the on-the-ground reality seen at empty local hospitals and unverified reports of overflowing morgues.
And yet, today, April 14, New York City added another 3,700 deaths to the COVID-19 death toll “who were presumed to have died of the coronavirus but had never tested positive”, as reported by the New York Times and others. This increased the US COVID-19 death toll by 17%. The deaths were reported as coming from hospitals, nursing homes and long-term care facilities from March 11 to April 13. The Times however sees this, like all mainstream media, as providing evidence of “shortcomings in testing”, not as complete fabrications made on the sole basis of symptoms, which is how the case determination was made.
Modeling questionable data
The computer model predicting the expected “disease curve” used by CDC’s Dr. Birx is a Bill Gates–funded model known as the IHME (Institute for Health Metrics and Evaluation) and is done at the University of Washington School of Medicine. This model, along with the Imperial College model used in the UK, has been shown to be wildly high off the mark in its US projections. The IHME model used the data from New York and New Jersey and applied it to the rest of the country, yielding a predicted death rate four times (121,000) greater than the “actual rate” (31,142) as of April 1. The model has been significantly revised several times since the beginning of the alleged pandemic in America, from 2 million to 200,000, to 121,00 and now 61,545 by August 4.
The US government–used Gates IHME model also seems to have dramatically overestimated the number of total US hospitalizations, ICU beds and ventilators needed, by 8, 6 and 40 times, respectively, according to scientist Ned Nikolov. It appears to have since been revised downward equally dramatically. The Gates model also overestimated the number of ICU beds needed in New York at least twice, by factors of three and four.

The model also has a 95% “uncertainty interval” said to be the result of limited or conflicting data. Covidtracking.com reports that the CDC is actually not reporting full data, and neither are the states: “Across the country, this reporting is also sparse. In short: it is impossible to assemble anything resembling the real statistics for hospitalizations, ICU admissions, or ventilator usage across the United States.” States are reporting different types of data, as noted.
Strikingly, in the case of Colorado, Covidtracking.com reports: “Cases include people who test positive for COVID-19 AND people who have symptoms of COVID-19 and are a close contact to someone who tested positive.” (Our emphasis) Similar to what Minnesota State Senator Dr. Scott Jensen has revealed to local media and FOX News, it appears a mere association with someone said to be “COVID-positive” is being counted as COVID cases.

The Gates IHME model also does not appear to represent a curve at all but a jagged leap. This “spikeyness” as well as the daily spikes in cases seen in China, Italy and Spain do not suggest a natural infection rate predicted by a smooth curve – but rather changes in accounting and reporting. Gates’s IHME claims their model’s performance and data notwithstanding, and the lack of evidence for this statement notwithstanding, that the lowering of the “curve” is confirmation that “social distancing works”. They continue to warn the public: ““Pandemic’s trajectory would change – and dramatically for the worse – if people ease up on social distancing.”
Navy Hospital Ships Remain Vacant
As of April 7, Politico reports that “The military-run hospitals at the Javits Center and onboard the USNS Comfort remain mostly empty — so far treating only 110 patients between them, Pentagon officials said Tuesday.” While the USNS Comfort’s capacity was previously reported at 1,000 beds, Politico and US Naval Institute News say now that the ship has a capacity of 500 beds but only 44 civilian patients, five of which are “COVID-positive”. A mere 66 patients were being treated at the “field hospital” set up at Javits Center. Nonetheless there are nearly 2,000 medical personnel at those locations.
As of April 2, the USNS Mercy docked off of Los Angeles has treated 15 patients out of a capacity of 1,000 beds. No COVID patients have been reported to have been on or treated on the Mercy. Both the Mercy and Comfort were supposed to treat non-corona patients to help with an overflow of patients, but the Comfort began accepting COVID patients. It is unclear how many if any were COVID-positive. The Mercy however has only had non-COVID patients, so one wonders how, as of April 14, seven crew members are reported to have tested positive for it.
It’s also been reported today that a Washington state “emergency field hospital” has been dismantled after treating no patients. Indeed, photos of field hospitals from around the country appear to be all virtually empty.
And yet all 50 states have been declared to be in a state of disaster.
Overcounts as Undercounts
Despite the phantom quality of the statistical picture of the “COVID” crisis, and the arguable over-reporting, overcounting or misreporting seen in these data, many reports have surfaced arguing that death counts have actually been underreported.
The US intelligence establishment just released a “classified” report charging China with a deliberate undercount. In Italy, it has been reported that COVID deaths in Bergamo province were understated because so many were dying at home. The same rationale has been argued to have occurred in the US, with the New York Times citing (but not attributing) New York City paramedics speculating that many New Yorkers may have died at home. Across the US, the Times says:
“The undercount is a result of inconsistent protocols, limited resources and a patchwork of decision making from one state or county to the next.
In many rural areas, coroners say they don’t have the tests they need to detect the disease. Doctors now believe that some deaths in February and early March, before the coronavirus reached epidemic levels in the United States, were likely misidentified as influenza or only described as pneumonia.”
Due to a lack of testing and awareness, the Times argues that many cases were missed:
“Early in the U.S. outbreak, virus-linked deaths may have been overlooked, hospital officials said. A late start to coronavirus testing hampered hospitals’ ability to detect the infection among patients with flulike symptoms in February and early March. Doctors at several hospitals reported treating pneumonia patients who eventually died before testing was available.”
Likewise, CNN’s Fareed Zakaria two days ago suggested that US death counts were overestimates due to a lack of testing. Like the Times, and the Stanford University scientists he cites, Zakaria suggests it is likely that “mild or asymptomatic cases” were missed and the lower fatality rate is due to this. Zakaria further states that up to 80% of alleged COVID-infected people have no symptoms, but does not cite his sources.
So, according to one of CNN’s most renowned journalists, the overcount simply missed all of those non-sick people who we somehow know are “carriers” (another unproven supposition). Go figure! In “Lock Step” with the rest of the corporate media, Zakaria also then concludes, again without any evidence, that “social distancing has done some good”.
A killer disease that is “mild or asymptomatic” is on its face a ridiculous proposition that all scientists should be addressing – but are not, and one that serves authoritarian objectives. The fact that viruses are all said to mutate is also a giveaway that the entire virus-vaccine paradigm, including vaccine and genetic vaccine technology are ruses. Because you can’t test or make a vaccine for a constantly-mutating virus. And you certainly can’t then “scale” that vaccine in up into a “one-size-fits-all” solution as is alleged to be possible.
As all of this weren’t enough to plague the least of skeptics, official talk has persisted in exaggerating reality in favor of the worst. We’d rather call it another fabrication. Despite all evidence to the contrary, White House Coronavirus Task Force lead Anthony Fauci insisted on April 13 that the situation had been “worse than we could have imagined”.
That’s an interesting statement, considering Fauci’s 2017 warning to incoming US President Donald Trump about the “inevitability of a ‘surprise outbreak’ of an “unknown infectious disease”. As reported by Business Insider:
“There is no question that there will be a challenge to the coming administration in the arena of infectious diseases,” Fauci said during a speech at Georgetown University, adding, “the thing we’re extraordinarily confident about is that we’re going to see this in the next few years.”
Fauci among others has also spoken of “second waves” and “rebounds” despite all evidence to the contrary, and despite an earlier March statement by Fauci to Congress that the disease did not “reinfect”.
At the April 7 Task Force press conference, Fauci warned that the virus will not go away. How he knows this is not known. Nevertheless he said: “[I]t’s gonna be different. Remember now, because this is not gonna disappear, so we’re going to have in place the capability of doing the things we talk about all the time on this stage: to identify, to isolate, to contact trace.” Fauci has also talked about using antibody tests for this.
And ultimately, tracking people appears to be the goal, despite the fact that no virus has been identified, isolated, or proven to cause a disease known as COVID-19. Nor is COVID conjecture confirmed by the reporting and statistics as outlined here.
Doctors and nurse confirm COVID overstatements
Inside the hospitals, some doctors and nurses have come forward to expose that the normal guidance for classification of deaths, “cause of death reporting” is now superseded by guidance that broadly links COVID to nearly anyone who comes into a hospital.
Dr. Annie Bukacek, a longtime Montana board-certified internal medicine physician has also come forward to blow the whistle on death rate exaggeration.
In a public statement, she said:
The CDC counts both true COVID-19 cases and speculative guesses of COVID-19 the same. They call it death by COVID-19. They automatically overestimate the real death numbers by their own admission.
The assumption of COVID-19 death can be made even without testing. Based on assumption alone the death can be reported to the public as another COVID-19 casualty. The March 24, 2020 National Vital Statistics System memo states, ‘The rules for coding and selection for underlying cause of death are expected to result in COVID-19 being the underlying cause more often than not.’ The CDC report of cases in the memo from yesterday states the death numbers are ‘preliminary and have not been confirmed.’
In other words, “Dying with COVID-19 is not the same as dying from COVID-19” but both are reported as COVID-19 deaths.
How many people have actually died from COVID-19 is anyone’s guess… but based on how death certificates are being filled out, you can be certain the number is substantially lower than what we are being told. Based on inaccurate, incomplete data people are being terrorized by fearmongers into relinquishing cherished freedoms.”
Minnesota State Senator Dr. Scott Jensen made headlines on Fox News, calling the April 2020 guidance for determining cause of death “ridiculous”. He also noted that hospitals will receive on average $13,000 in Medicare payments per COVID patient and $39,000 per patient requiring a ventilator. The practice of exorbitant Medicare billing per ventilator has already been noted as a concern by the US Department of Health and Human Services (DHHS). In a 2016 document, it stated that Medicare paid 85 times more claims for noninvasive pressure support ventilators in 2015 than in 2009.
And due to a decision by DHHS to allocate the first $30 billion of CARES funds by historical share of Medicare billings, not on current need, some states, such as Minnesota, Nebraska and Montana, are reportedly receiving more than $300,000 per COVID case from Medicare, Keiser Health News reports. New York is receiving $12,000 per case while Florida is getting $132,000 per case.
So there is a clearly established financial incentive for hospitals to declare COVID cases. And that may also be a legitimate threat to patients who are told they have COVID. STAT News reports: “some critical care physicians are questioning the widespread use of the breathing machines for Covid-19 patients, saying that large numbers of patients could instead be treated with less intensive respiratory support.”
A 2010 HealthDay report cited a University of Pittsburgh study of seven years of Medicare data showing that all elders on mechanical ventilators either die within the year or are very disabled by the invasive treatment:
“Unfortunately, 70 percent of elders who receive mechanical ventilation will not survive the year. And the 30 percent who are strong enough to survive will be very disabled,” study author Dr. Amber Barnato, an associate professor of medicine at the University of Pittsburgh, said in an American Thoracic Society news release.”
A Utah ICU nurse with 30 years of experience also has anonymously come forward to reveal pro-COVID bias in diagnosing cases: “You basically treat the patient as if they have it, until you find out they don’t… If a patient dies, if they are COVID-positive, you put COVID as the cause of death.”
She further notes the case of a terminally ill patient who was given a COVID test:
“That’s bizarre that you would do that on a hospice patient, but they would get a COVID test positive. That person wouldn’t die of their terminal disease. They died of COVID. This is what is happening – that’s the issue, that our hands are tied…. We can’t disclose this technically to anyone, or you are breaking federal law.”
The nurse further noted the sacrifice of preventative care, and care of patients in need from other causes:
“All preventative care at this moment is shut down. No one is getting preventative care. I did hear a conversation of two cardiologists basically saying there are probably a lot of people who are just staying home and having silent heart attacks in their home.”
“And the other issue is organic donation… donor services have been nearly completely shut down at this point in placing organs… I can’t tolerate the dishonesty and lack of integrity and the giving into the emotional side of it. We are acting as if everyone has end-stage AIDS. (Our emphasis)
To make matters worse for the general public who might have a health emergency, amidst the manufactured “crisis”, thousands of US hospital workers are reported to have been “furloughed”, laid off or had hours reduced as “routine patients have dropped off”. (Disingenuous language attributing these developments to basic supply and demand is rife in media right now: “demand has dropped”.) In fact, the public has been told by authorities, specifically, the Surgeon General Jerome Adams to postpone or not seek medical care and to stay at home. The Daily Mail reports that doctors have been asked to accept pay cuts of up to 70%, and cites a statistical model produced in association with the American Academy of Family Physicians suggesting that by the end of April, “almost 20,000 family physicians could be underemployed, reassigned or out of a job altogether.”
Here’s Jessica, a laid-off nurse from Cleveland. She says, “I work at an outpatient clinic. But we have hardly any patients so I’m not working. My friends in the ICU that I used to work in, they’re hardly working. They’re getting canceled shifts. And this is big hospitals in the Cleveland area. Numbers are down.” Cleveland Clinic has one case, noted in the interview.
Private medical practices have been forced closed, and dental service has basically stopped. In the UK, elderly individuals and the parents of sick children have been asked to sign “do not resuscitate” orders so as to make room for alleged COVID patients. In the US, an eyebrow-raising March 25 Washington Post report revealed that hospitals as of late March were “consider[ing] universal do-not-resuscitate’ orders for coronavirus patients”:
Several large hospital systems — Atrium Health in the Carolinas, Geisinger in Pennsylvania and regional Kaiser Permanente networks — are looking at guidelines that would allow doctors to override the wishes of the coronavirus patient or family members on a case-by-case basis due to the risk to doctors and nurses, or a shortage of protective equipment, say ethicists and doctors involved in those conversations. But they would stop short of imposing a do-not-resuscitate order on every coronavirus patient.
The report also noted that Northwestern Memorial Hospital in Chicago and George Washington University Hospital in Washington, DC were considering a similar policy, even though they are not sure if it is legal. The Post also reported:
“As cases mount amid a national shortage of personal protective equipment, or PPE, hospitals are beginning to implement emergency measures that will either minimize, modify or completely stop the use of certain procedures on patients with covid-19.
Some of the most anxiety-provoking minutes in a health-care worker’s day involve participating in procedures that send virus-laced droplets from a patient’s airways all over the room.
These include endoscopies, bronchoscopies and other procedures in which tubes or cameras are sent down the throat and are routine in ICUs to look for bleeds or examine the inside of the lungs.
Changing or eliminating those protocols is likely to decrease some patients’ chances for survival. But hospital administrators and doctors say the measures are necessary to save the most lives.”
Both the denial of medical care and the euthanasia orders are shocking and violate natural, constitutional, human rights and international laws.
Conversations such as these raise the further questions of what is happening in nursing homes. From the beginning of the coronavirus event, people were told to avoid nursing homes, after which several mass COVID deaths from nursing homes were reported. The New York City addition of 3,700 deaths included deaths from nursing homes and long-term care facilities, as noted.
Media fabrications
Finally, intrepid social media posters have exposed many media “anomalies” in COVID death reporting, just a few of which we mention here:
A photo of the same boy was found to represent two different boy COVID victims in two different countries, Britain and Portugal, by two UK presses:

In a third UK publication, the boy is shown as a Belgian female coronavirus victim:

Further, the BBC has reportedly misrepresented mass graves at New York City’s Hart Island as coronavirus mass graves, despite the fact that New York Mayor Bill de Blasio stated that the graves are full of bodies from all deaths. Nonetheless the mayor set up the disinformation by increasing the number of burials at this site by a factor of three.
Finally, we end with an April 7 report from USA Today‘s Joel Shannon, who should lose all journalistic credibility. USA Today reports that total US COVID fatalities are “more than the total battlefield fatalities from six combined wars.” Setting aside what a “combined war” is, the USA Today piece features a video alleging to show how “novel” coronavirus attacks the body and becomes fatal – or is asymptomatic. The whole disease sequence – again, unless you are asymptomatic, a claim which does not pass basic scientific muster – has never ever been proven.
The next part of this report will address the World Health Organization’s prior, similar use of accounting changes to create the appearance of a pandemic, as well as their funding by the Bill and Melinda Gates Foundation and vaccine manufacturers.
Finally, since this development is occurring based on high COVID case and death counts, we include this update:
Army Times is reporting that “With empty beds at the Javits Center and on the Comfort, uniformed health workers are going straight into NYC hospitals”. They will now be stationed in hospitals. In addition, according to Lt. Col. Leslie Curtis, the 9th Field Hospitals chief nursing officer, there are more than two dozen teams “going out on missions to support emergency response”. (Quote is Army Times’s reporting, not a direct quote.)
Further:
[H]ealth care workers are taking every precaution to stop the spread, donning the same complement of personal protective gear for each patient, whether that person is specifically being treated for COVID-19 or not.
“We’re treating everyone as if they’re COVID positive,” she [Col. Jennifer Ratcliff, who commands the 927th Aerospace Medical Squadron] said, because it’s safer to assume, given the tens of thousands of cases in New York City. “It’s more likely that someone is COVID positive than COVID negative.”
New York appears to be past its COVID peak, but the army has decided it’s infected.
4 Comments
https://jtremaine.wordpress.com/2020/04/14/watch-united-states-is-over-trump-hands-it-over-to-f-e-m-a-on-youtube/
“It’s like déjà vu all over again.”
Just like my study of 9-11-01 since 9-11-01
Garbage, lie-cheat-steal data and twisting of words and meanings that no one can make sense of.
To me, President Trump has from the beginning of his presidency up until this very day has been appointing creatures of the so-called “Deep State” to be part of his closest advisors and cabinet members and special task force members. Some say the president is just playing “5 D chess.”
The president’s policy moves to act upon false and misleading data from his team’s “top experts and medical scientist” regarding this “coronavirus” or its nonsense synonym “COVID 19” has probably permanently destroyed the USA constitutional republic forever and destroyed the livelihoods of a large proportion of its middle and lower income workers, as well as the possession of their abodes.
I cannot think of any redeeming “5 D Chess” strategies of his that could make all of the world’s people who have been wiped out by this mother of all false flag events forgive him and his trusted inner circle of advisors, but then this movie and all this play acting ain’t quite over.
The only shred of hope I still hold about the president relates to the current conspiracy theory that every poor and ruined person in every country could also forgive him. Maybe the living children victims of a worldwide human trafficking and child sexual and satanic ritual abuse and sacrifice cabal really are about to be rescued on to the Mercy in the port of Los Angeles and the Comfort in the port of New York city, this to happen within the next two weeks. Maybe the ring leaders of this worldwide human trafficking and child sexual abuse EVIL INCARNATE entity will be apprehended and incarcerated forever without bail and their names and faces and identities will be shown to the world as will photographs and videos of the poor abused children who are said to be in cages in the underground tunnels of Los Angeles and New York City.
Romans 8:28
The reason for this declared “pandemic” is the following- first think back on how many “official” pandemics there were from say 1960-2005. Now how many “declared” pandemics have there been since that time.
Understand this recent timeline and what has changed.
In 2005 the WHO, the organization that “decides” what is and what is not a pandemic, changed the way it was funded. It went from a member funded global health agency to one where private interests now contributed the majority of it’s funds. This meant in particular that large pharmaceutical companies and investors connected to them now became the primary donors to the WHO- these are commonly referred to as Public-Private-Partnerships (PPP’s). As a part of this arrangement these new funding entities demanded a seat at the table of the executive committees who make all sorts of policy decisions at the WHO. The WHO emergency executive committees are the ones responsible for “officially” declaring that there is a global pandemic.
In 2007 the WHO changed it’s specific definition as to what qualifies as a global pandemic.
The old definition was as follows: “a pandemic is an infection of global proportions and with a high mortality rate”- that definition was changed in 2007 to the more general and vague “a pandemic is an infection of global proportions.” Mortality rate was excluded. This relaxing of the definition allowed for a more liberal interpretation of what was or could be considered in officialdom a global pandemic. This is not just a mincing of words.
Why this is so vital to understand is that once a pandemic is “officially” declared mechanisms in place and done through the WHO kick into gear designed to deal with this newly declared “global pandemic.” And who might you ask decides the direction and manner of these mechanisms? The executive committee itself which is now loaded with various representatives of those large pharmaceutical interests which will directly benefit from these global pandemics.
One of THE main outcomes in these PPP’s is that the large amounts of funding that goes to combat these now seasonal “global pandemics” gets funneled directly into the coffers of the big business interests who decide what is a pandemic and how it should be dealt with- meaning funding that goes towards research and development that will now directly benefit those companies who “donate” to the WHO- primarily Big Pharma.
“When a donor gives money, for example, the pharmaceutical industry, these representatives request to be present on the expert committees of the different [WHO] programs. There is a serious conflict of interest. It happened with the H1N1 epidemic, potential vaccine and drug manufacturers, like Tamiflú, were sitting on the committee that was deciding whether to launch an epidemic or not, obviously [the pharmaceutical companies] pushed for the epidemic to start and give a global alarm because they were going to have an impressive market. ”
– German Velásquez, the creator of the Health Economics and Drug Financing Unit of the World Health Organization and former Director of its Secretariat for Public Health, Innovation and Intellectual Property
https://fightnwo2010.wordpress.com/2020/05/10/oppose-hr-6666-the-tres-act-please-act-immediately-we-the-people-your-voice-in-our-government/