When #Plandemic Models Fail, Invent “Hidden Outbreaks”
Guest post
If it’s not deadly, it must be more widespread
As people are now aware from Our previous reporting that the case and death counts for the alleged COVID-19 disease have been fabricated and inflated in many (and likely most) countries, and especially in the US, establishment operatives have done their best to end run this information to suit their illegal universal testing and vaccination agenda and extend their illegal lockdowns. Mainstream media reports that new non-peer-reviewed studies suggest the fatality rate of COVID is much lower than originally modeled, not because of the over-reaching government guidance to classify non-COVID cases as COVID cases, which medical staff and the official statistics have corroborated, but because “asymptomatic infections” were “missed”.
In other words, “new coronavirus” is less deadly only because it is much more widespread in asymptomatic form, they say, and therefore the death numbers must be compared against a wider population assumed to be infected. But the idea that coronavirus is widespread in “asymptomatic” form is not proven. And as just noted, the overinflated mortality rates were already explained by the “liberal approach” taken by governments in classifying other deaths as COVID deaths. In suggesting that great numbers of people are actually “infected”, the #plandemic criminals are not only controlling the opposition narrative, but they are further faking, and artificially increasing, an already fake infection rate and expanding the pandemic timeframe to reflect an earlier outbreak. They are doing it to suit the medical surveillance agenda – not to argue that lockdowns are unnecessary.
The low COVID death rate information was most recently “hot miked” in the White House Press room late last week by Fox News before a Trump Coronavirus Press Briefing. Two men prepping for the event referred to an unpublished USC study alleging a massive infection rate roughly 30 to 60 times higher than currently measured:
“They found that there were 7,000 cases in California. But they really believe that where were anywhere from 221,000 to 442,000 people who were infected…. So that makes it 0.1 to 0.3.… So that suggests the case fatality rate is what? A tenth of what it seems it be. Puts it right in line with the flu. … [Other man: So it’s a hoax?] I don’t think it was a hoax.”
Of course, it couldn’t be a complete and utter hoax.
Unfortunately, many commenters in alternative media including Dell Bigtree, whistleblowing ER docs and even Senator Rand Paul are forwarding studies such as this to promote idea that the virus is widespread but mild in order to prove COVID is not dangerous and not worthy of shutting down all of society – which is well and good. We fully support #ReopenAmericaNow. But unfortunately it is mistaken.
The evidence offered of a high asymptomatic infection rate is very flimsy and not at all peer-reviewed. In reality, it’s just more cheap accounting tricks – or rather, as Bill Gates is fond to do, lying with statistics.
Manufacturing “facts”
Dr. Anthony Fauci himself first suggested that a high number of asymptomatic cases would lower the mortality rate in a late-February New England Journal of Medicine editorial:
“If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.” (emphasis ours)
It’s worth noting that despite this statement, Fauci continued to tell the public via the Daily Show in late March: “[T]he mortality of seasonal flu…is about 0.1%. … But the mortality of this is about 10 times that. It’s at least 1%.”
Fauci’s assumption about “asymptomatic or minimally symptomatic cases” refers to a February Chinese study which itself refers to WHO guidance asserting that 81% of people “have uncomplicated or mild illness”. The WHO’s figure derives from another early February Chinese study, this one an epidemiological study from the Chinese CDC, presumably the largest done at the time, in which the 81% does not refer to asymptomatic carriers but to “mild” COVID cases including “mild pneumonias”. (bold, italics ours)
Here is the version of the Chinese CDC study referenced by the WHO:
“A total of 72,314 patient records – 44 672 (61.8%) confirmed cases, 16,186 (22.4%) suspected cases, 10,567 (14.6%) clinical diagnosed cases (Hubei only), and 889 asymptomatic cases (1.2%) – contributed data for the analysis. Among confirmed cases, most were aged 30-79 years (86.6%), diagnosed in Hubei (74.7%), and considered mild/mild pneumonia (80.9%).” (italics/bold ours)
“Among confirmed cases, most were aged 30–79 years (86.6%), diagnosed in Hubei (74.7%), and considered mild (80.9%).” (bold ours)
Version printed at JAMA:
“Among a total of 72,314 case records, 44,672 were classified as confirmed cases of COVID-19 (62%; diagnosis based on positive viral nucleic acid test result on throat swab samples), 16,186 as suspected cases (22%; diagnosis based on symptoms and exposures only, no test was performed because testing capacity is insufficient to meet current needs), 10,567 as clinically diagnosed cases (15%; this designation is being used in Hubei Province only; in these cases, no test was performed but diagnosis was made based on symptoms, exposures, and presence of lung imaging features consistent with coronavirus pneumonia), and 889 as asymptomatic cases (1%; diagnosis by positive viral nucleic acid test result but lacking typical symptoms including fever, dry cough, and fatigue)…
· Spectrum of disease (N = 44 415)
- Mild: 81% (36 160 cases)
- Severe: 14% (6168 cases)
- Critical: 5% (2087 cases)
“Most cases were classified as mild (81%; ie, nonpneumonia and mild pneumonia).” (bold, italics ours)
What this study really said is that only 889 out of 45,561 lab-confirmed (nucleic acid–tested) cases were asymptomatic – again the questionable reliability of these tests notwithstanding – which is actually 2% of tested cases, not 81% of confirmed cases. The study in fact considers asymptomatic cases to be only 1% of all presumed cases.
What the WHO and Fauci have done is to use the Chinese figure for mild symptomatic cases including cases of pneumonia and falsely ascribe it to “asymptomatic” cases. This makes COVID appear more “infectious” despite a lower fatality rate and seems to have provided basis for conjecture about “asymptomatic carriers” fueling the pandemic.
Testing and tracing, i.e., “biosurveillance” companies as well as liberty-crushing governments stand to benefit greatly from the idea that there are a vast number of unidentified COVID “carriers”.
Meet the new unscientific models, same as the old unscientific models
The only way the political-scientific establishment admits COVID is not very deadly is by reverse-engineering facts on the ground via new models: The new alleged virus infected many more people in the US far earlier than anyone thought, and these “asymptomatic carriers” have been actually “fueling the pandemic” in “hidden outbreaks”, Discover Magazine conjectured in March. Many people are already repeating this claim, with no verification.
This charge has been made against presumed asymptomatic carriers in China and Japan, but the studies of alleged “carriers” are: based on more mathematical, so-called “epidemiological” modeling, inconsistent and largely not peer-reviewed. We need to remind here: mathematical modeling is not science, but exercises based on assumptions. Asymptomatic carriers have been found by these mathematical models to be responsible from anywhere from 15% to 59% and 86% of cases internationally, according to different studies, two of which were not peer-reviewed and another with disclosed conflicts of interest.
For example, about the mathematical model used to estimate that 59% of asymptomatic cases fueled the alleged pandemic in Wuhan, China, Gerardo Chowell, a mathematical epidemiologist at Georgia State University, has noted in the journal Nature, “By assuming there is homogeneous mixing, the model probably overestimates the transmission rate and exaggerates the number of infections with mild or no symptoms.” Homogenous mixing refers to the very unlikely scenario of random interaction with the public at large vs. interaction among one’s known circle and locations. So, that’s a false assumption built into the model.
And though we have been told the entire reason for the lockdown was person-to-person transmission, in fact, according to Jeffrey Shaman of Columbia University’s Mailman School of Public Health:
“The reality is, we don’t really know how respiratory viruses are transmitted. We know how they can be, [but] we don’t actually know how they are. The same is true for the novel coronavirus. We think it spreads through droplets, but there is still too little evidence to say for sure.”
(It’s worth remembering that no one has shown how viruses can jump from animals to humans either, or conjectured as to why our pets are not in danger from coronavirus but humans are.)
Shaman noted what should be an insurmountable caveat in this same Discover report, despite advancing an epidemiological computer model “study” in mid-March, with a list of international contributors that includes the Bill Gates–funded Imperial College team asserting that 86% of cases in China were “undocumented” drivers of COVID. The study uses a “model-inference framework” and further admits there are “many uncertainties regarding pathogen transmissibility and virulence”.
One wonders what other transmission assumptions that model made if scientists don’t know how alleged respiratory viruses are transmitted. Well, they just assumed something anyway: for example, that asymptomatic carriers are half as contagious as “documented infections”. Sure, there’s probably a math equation behind that that makes sense. But is it correct? Or is it just an assumption? How could asymptomatic carriers be driving a pandemic when they are only half as infectious as those who are alleged to have a full-blown infection? And in this “study,” scientists also assume that mask wearing, school closures and restricted travel have already “slowed the spread” of the alleged virus, which are also all pure conjecture.
ProPublica, however, continued to report in a similar article alleging “asymptomatic carriers” were driving the COVID disease: “The disease IS spread by liquid “droplets.”
What’s really pushed the new fake narrative of ‘missed asymptomatic infections’ to the public fore, however, have been similar models advanced by Stanford University scientists. It is interesting to note that Stanford University’s science departments have long been associated with the US government, military and intelligence.
Stanford University professor of medicine, epidemiology and “population health” as well as “biomedical data science” John Ioannidis, one of the top 10 most cited scientists in the world according to his CV, was one of the first to argue, in STAT on March 17, that a lack of testing may have missed infections. Alternative media has somehow taken this man to be a hero, but in fact, he supports a widespread testing agenda based on the same idea of asymptomatic carriers spreading the ‘disease’.
“The data collected so far on how many people are infected and how the epidemic is evolving are utterly unreliable. Given the limited testing to date, some deaths and probably the vast majority of infections due to SARS-CoV-2 are being missed. We don’t know if we are failing to capture infections by a factor of three or 300.” (emphasis ours)
As mentioned in our prior post, CNN host Fareed Zakaria was also pushing the ‘missed infections’ narrative, which the ‘inadequate testing’ narrative sets up, as soon as the earlier Gates-funded IHME/Imperial College computer models were perceived to be failures. In mid-March he said:
“A group of Stanford scholars believe[s] that the basic reason estimates of deaths were revised downwards is because without an understanding of how the virus spreads and without widespread testing from the start, we didn’t realize how many mild or asymptomatic cases there would be. That means the denominator – those who have been infected – could be much larger than initial estimates, and therefore the fatality rate for COVID-19 is actually much lower.” (emphasis ours)
In his report, Zakaria further refers to a March 24 Wall Street Journal editorial by Stanford University professors of medicine, Drs. Eran Bendavid and Jay Bhattacharya, which asked, “Is coronavirus as deadly as they say?” As re-reported by the Daily Wire, they reiterated the same assumption of a much larger number of “actual infections”:
“The true fatality rate is the portion of those infected who die, not the deaths from identified positive cases… If the number of actual infections is much larger than the number of cases—orders of magnitude larger—then the true fatality rate is much lower as well. That’s not only plausible but likely based on what we know so far.”
After this talking point thoroughly suffused media reports in mid- to late March, several new studies surfaced, two from California and a new model from a private institute operating out of Northeastern University, for which we have yet to find a primary source and reported only in the New York Times, alleging that “Hidden Outbreaks Spread Through U.S. Cities Far Earlier Than Americans Knew, Estimates Say”.
The first and most publicized of these studies is by the same doctors cited by Fareed Zakaria, Drs. Eran Bendavid and Jay Bhattacharya of Stanford. The approach underlying these studies, as cited from their WSJ op-ed, is basically to test a target population and then extrapolate that to a larger or entire population. Discussing the northern Italian town of Vò, the scientists took a small town that already had an “early outbreak” and extrapolated that to the entire province of Padua:
“On March 6, all 3,300 people of Vò were tested, and 90 were positive, a prevalence of 2.7%. Applying that prevalence to the whole province (population 955,000), which had 198 reported cases, suggests there were actually 26,000 infections at that time. That’s more than 130-fold the number of actual reported cases. Since Italy’s case fatality rate of 8% is estimated using the confirmed cases, the real fatality rate could in fact be closer to 0.06%.”
Of course, disease prevalence cannot be assumed to be the same everywhere. Yet here, a whole province is assumed to have the same disease prevalence as one area known for having an outbreak. In the same op-ed, these Stanford scientists use a similar analogy to extrapolate from NBA players, a group with a very suspiciously high COVID rate, to the cities that host NBA teams. Several commenters have called this basic extrapolation “junk science”.
Nonetheless the Stanford scientists proceeded from junk science conjecture to real junk science that has now been cited on the Senate floor by Rand Paul and publicized as a legitimate study by Dell Bigtree and others, as noted.
The Stanford scientists’ study, which was not peer-reviewed, according to the Guardian, “tested samples from 3,330 people in Santa Clara County and found the virus was 50 to 85 times more common than official figures indicated.” Even counting the dead, the Guardian reports that the rate of infection was actually 3%. Elsewhere it has been revised upward to 4.16%.
“At the time of the study, Santa Clara County had 1,094 confirmed cases of Covid-19, resulting in 50 deaths. But based on the rate of participants who have antibodies, the study estimates it is likely that between 48,000 and 81,000 people had been infected in Santa Clara County by early April.”
That’s between 44 and 74 times higher than actually confirmed, and again these confirmations are themselves not proven to be accurate. As reported by the Guardian, there were many concerns about the Stanford study’s sample and statistical analysis: “The biggest criticism was that it estimated cases for the whole county’s population based on detecting only 50 positives out of 3,300 people sampled. And since the tests had a false positive rate in one assessment of two out of 371, critics argued all the Covid-19 cases detected by the tests in Santa Clara could conceivably have been false positives.”
Statisticians looking at the epidemiological study quickly called it ‘junk’ on social media. As further reported by the Guardian:
“I think the authors of the above-linked paper owe us all an apology,” wrote Andrew Gelman, director of the applied statistics center at Columbia University, who has written numerous books on teaching statistical methods. “We wasted time and effort discussing this paper whose main selling point was some numbers that were essentially the product of a statistical error.” …
The author and biotech investor Peter Kolchinsky tweeted that the “flaws with this study could trick you into thinking that getting shot in the head has a low chance of killing you”.
Not uncoincidentally, the San Jose Mercury News reported at the same time as the Santa Clara study, that the very first US COVID death was a San Jose woman who died February 6, and that two other unnamed victims were also early, previously unreported COVID deaths. It appears that local officials are also now testing the dead to scare up more COVID deaths, and more importantly, to bolster the idea that in those early weeks in which federal officials were said to be dithering, cases and deaths were missed.
The San Francisco Chronicle further reported that the coronavirus caused the woman’s heart to rupture, though she is also said to have been mildly obese with mild pneumonia. The autopsy was started February 7 but not completed until now (late April). And further, the actual autopsy notes that no “immunohistological evidence of SARS-CoV-2 was found in [the woman’s] heart, trachea, lung or intestines” but that the diagnosis of the presence of virus was made by the detection of viral RNA. In other words, they didn’t find a whole dead virus, just some RNA said to be attributed to it. And this appears to be how the COVID death determination was made.
The Mercury News nonetheless conjectured: “The deaths — which occurred weeks before the first publicly reported coronavirus fatality in the county — raise questions about the true scope of the virus’s toll in the Bay Area.”
Another study from Los Angeles done by USC offers a similarly inflated infection rate based on serology tests, but this study is not available to review online and has not been peer-reviewed either. It was however the “study” hot-miked by Fox News before the Coronavirus Press Conference last week, and it appears to use the same basic extrapolation method as the Santa Clara County study. As also reported by the Guardian:
“[A]ccording to the team’s press spokesperson, the researchers estimate based on 863 tests that as many as 5.6% of adults in the county, or 442,000 people, had already had the virus by early April. The number of confirmed Covid-19 cases in the county at the time was only 7,994.”
That’s 55 times higher than previously reported via already questionable case confirmations. The idea is to get you talking about the undercounted cases again, not the potential or likely overcounts in the original 7,994, which as we have noted in prior reporting, are not substantiated.
Significantly, the Guardian reports that none of the California studies’ authors’ responded to its requests for comments in light of the criticism from other scientists and peers.
As for other “Hidden Outbreaks” in the US, the New York Times reports on a new, unpublished, unreviewed Northeastern University mathematical computer model for which we have absolutely no information, stating: “In five major U.S. cities, as of March 1 there were only 23 confirmed cases of coronavirus. But according to the Northeastern model, there could have actually been about 28,000 infections in those cities by then.”
The unpublished model asserts that Boston and Seattle actually had 2,300 cases as of the same date, Chicago had 3,300 cases, San Francisco had 9,300 cases and New York had 10,700 cases. And, they add that these are only median estimates, meaning: “The true number of infections could have been substantially higher or lower than shown here.”
The true number infections, according to the repeated narrative, were due to “asymptomatic carriers” plus slow official action including a lack of testing: “Unseen carriers of the disease, many of them with mild symptoms or none at all, can still spread the virus. For that reason, by the time leaders in many cities and states took action, it was already too late to slow the initial spread.”
““We weren’t testing, and if you’re not testing you don’t know,” Dr. [Adriana] Heguy [director of the Genome Technology Center at New York University’s Grossman School of Medicine] said. The new estimates suggesting that thousands of infections were spreading silently in the first months of the year “don’t seem surprising at all,” she said.”
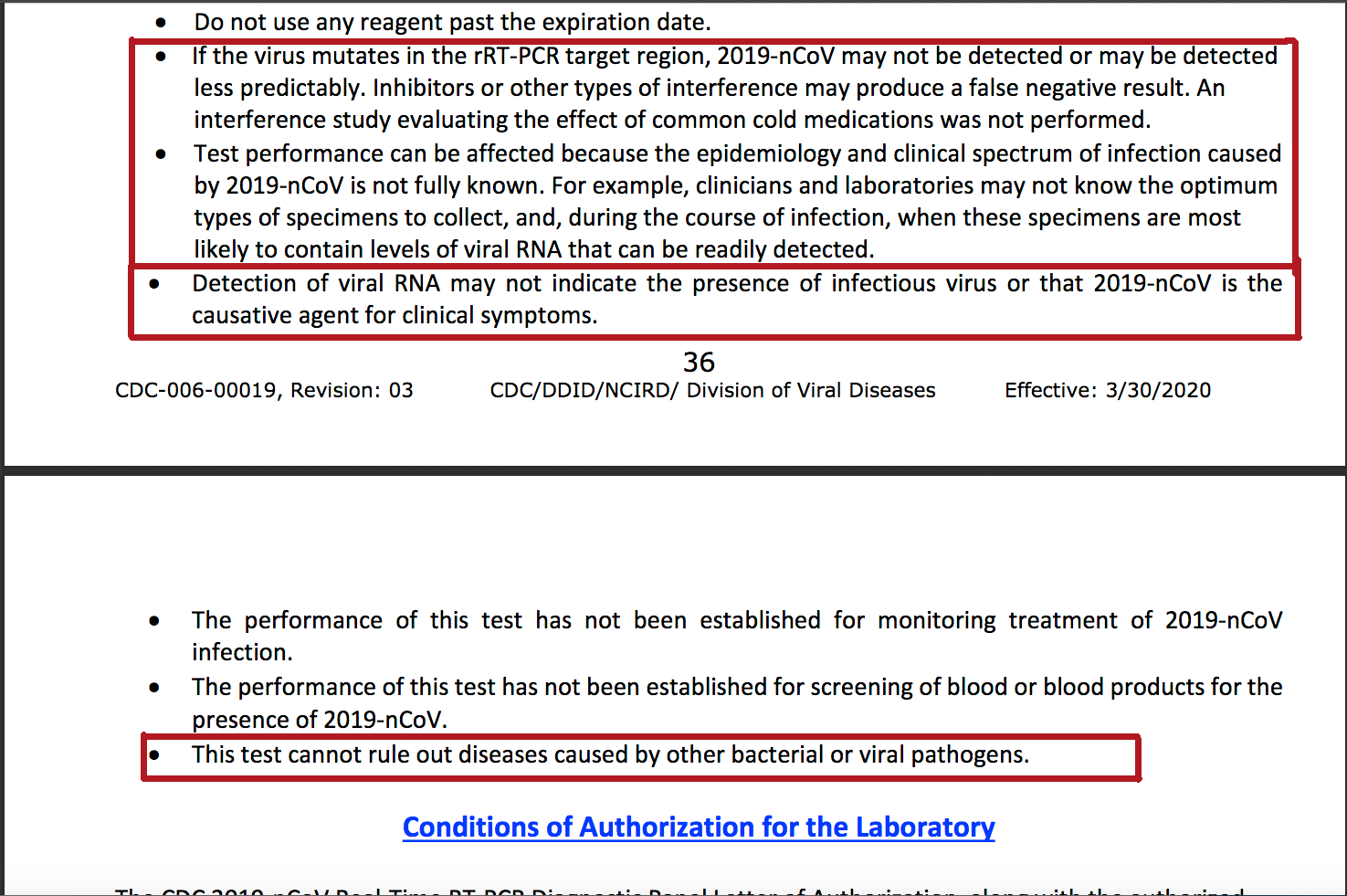
Never mind that the tests to date, PCR tests, are still unable, by the CDC’s own admission in its instructions, to accurately test for the alleged virus. And never mind that not all cases were lab-confirmed cases, but merely “suspected”, “assumed” or “probable”.
And further remember: The only reason alleged COVID cases in New York and New Jersey rose, indeed, spiked, by hundreds in a day on several occasions, was due to an increase in testing, as was well reported at the time. This was also the case as reported from China, Spain and Italy as well.
It seems one surefire way to “get COVID” is simply to be tested for it. But of course, some medical professional could just assume you have it, as the WHO and CDC have directed them to do.
Meet the new bad tests, not much different than the old bad tests
The Guardian reports that both California studies noted above “used an antibody test made by Premier Biotech Inc. that has not been approved by the FDA and comes with an acknowledgment that it can record false positives.” As noted, the tests used in the Stanford study were antibody, or serology, tests that appear to have had a one-in-two false-positive rate. Well-known scientists have been critical of the antibody tests, “hundreds of which have emerged on the world market in recent weeks”, according to Reuters. None of them currently have FDA approval but have been fast-tracked without review or regulation. Some of them are “a disaster”, Roche CEO Severin Schwan told Reuters.
And, like the PCR tests, the antibody tests can’t actually detect any virus. (They are called “presumptive tests”.) Here’s WebMD on “COVID” antibody tests:
“The antibody test isn’t checking for the virus itself. Instead, it looks to see whether your immune system – your body’s defense against illness – has responded to the infection. … Keep in mind that current antibody tests can’t tell you if you’re immune to COVID-19. That’s because we don’t know how long these antibodies might protect you against the coronavirus. And these tests shouldn’t be used to diagnose the virus.” (emphasis ours)
The New York Times, alongside a pro-testing op-ed written by a Harvard economist (many of whom have been spouting shocking prescriptions for the long-term continuance of the #illegallockdowns in recent weeks), noted in “Coronavirus Antibody Tests: Can You Trust the Results?” that “A team of [over 50] scientists worked around the clock to evaluate 14 antibody tests. A few [3] worked as advertised. Most did not.”
Further:
“Four of the tests produced false-positive rates ranging from 11 percent to 16 percent; many of the rest hovered around 5 percent.
“Those numbers are just unacceptable,” said Scott Hensley, a microbiologist at the University of Pennsylvania. “The tone of the paper is, ‘Look how good the tests are.’ But I look at these data, and I don’t really see that.”
The proportion of people in the United States who have been exposed to the coronavirus is likely to be 5 percent or less, Dr. Hensley said. “If your kit has a 3 percent false-positive, how do you interpret that? It’s basically impossible,” he said. “If your kit has 14 percent false positive, it’s useless.””
And, because the proposed “rapid antibody” tests are essentially like PCR tests in that they only give a yes-no response, one wonders why ELISA tests, which allegedly indicate the amount of antibody present quantitatively (they likely do not) are not used exclusively in tests being sold to the public and local governments. ELISA tests will be used in an upcoming NIAID serology study of 10,000 volunteers run by Dr. Fauci’s lab.
According to a Medscape report on the antibody tests, Kelly Wroblewski, director of infectious diseases at the Association of Public Health Laboratories (APHL), said in a news conference on April 14, “These tests create more uncertainty than before. Having many inaccurate tests is worse than having no tests at all.”
A bigger rub, however, is this: Only a small percentage of the population is said to even have antibodies, and the antibodies are said not to provide immunity from the alleged COVID disease.
Arthur Reingold, a UC Berkeley professor of epidemiology cited in the Guardian, has said about the serology tests:
“The idea this would be a passport to going safely back to work and getting us up and running has two constraints: we do not know if antibodies protect you and for how long, and a very small percentage of the population even has antibodies.”
The WHO’s “technical lead for COVID-19”, Dr. Maria Van Kerkhove, further noted that “even if tests showed a person had antibodies, it did not prove that they were immune.” She told the Guardian, “There are a lot of countries that are suggesting using rapid diagnostic serological tests to be able to capture what they think will be a measure of immunity. Right now, we have no evidence that the use of a serological test can show that an individual has immunity or is protected from reinfection.”
The WHO head has also echoed this point in recent days, that only a few people have “developed” COVID antibodies, with its head still insisting “the worst is yet to come”. From the Guardian:
“Only a tiny proportion of the global population – maybe as few as 2% or 3% – appear to have antibodies in the blood showing they have been infected with Covid-19, according to the World Health Organization, a finding that bodes ill for hopes that herd immunity will ease the exit from lockdown.”
Antibody tests from France and Germany cited by Van Kerkhove, however, have shown that “up to 14%” of people in those countries had antibodies for the alleged virus.
So, what are governments and so-called public health agencies doing with these antibody tests? Why does immunity need to be proven – especially immunity to a disease that has not been proven to exist or to have killed anyone in significant numbers? Moreover, if the disease is so widespread and this widespread infection is fueling the pandemic, how could so few have antibodies? What is the point of looking for antibodies that few are presumed to have?
Scientists have claimed that antibodies don’t necessarily prove immunity because we don’t know how immunity from COVID works in terms of how antibodies interact with the alleged virus. Critical researchers have noted that science has not even proven that the antigen-antibody model of immunity even exists as such. So again: why the tests?
The reason the establishment is insisting on these farcical tests that don’t accurately test anything is to precisely to falsely confirm, i.e., fake, what the WHO and CDC would like to prove but cannot: there is a large, dangerous silent outbreak that is a risk to most people. If most people test negative for COVID antibodies, which they will, in far larger numbers than the PCR tests “confirmed” COVID, they will be said to remain at risk or a risk in need of treatment. The WHO and CDC, who have already invested in and get a vast majority of their funding from vaccine investors and manufacturers, are the ones mandating “proof of immunity”, which is a conjecture that is not only unscientific but breaks all recognized human rights laws to one’s person including the Nuremberg code. So, the manufactured “need” to vaccinate is one reason for insisting on more dubious testing.
Large-scale surveillance is the other reason. As the Medscape article suggests, the information derived from antibody tests “could be valuable to epidemiologists and policy makers”: “States are looking at ways they can integrate reliable serologic tests for surveillance,” according to APHL’s chief program officer Eric Blank.
Epidemiologists can use the tests to invent hidden outbreaks based on basic extrapolation to create an overwhelming mass of asymptomatic carriers and thus an extended outbreak timeline, such as the Guardian asserts in “Coronavirus was killing Americans weeks earlier than thought”. States and politicians will use the bloated, phony results to justify their #illegallockdowns, perform “syndromic surveillance” and “contact tracing” of crowds and individuals, and also to justify the manufactured need for “immunity passports” to continue to illegally restrict and control people’s behavior. And, as one doctor posting to Medscape also admitted, serology tests can be “useful in modifying the behavior” of patients who test negative, so that they better practice “social distancing” and “hygiene”.
This is just the sweet spot you want to be in if you’re insane and your business is manufacturing fake disease – a disease must not be so widespread as to invoke “herd immunity”, but wide enough so that restrictions on freedom and “treatments” can be sold as aids to the captive public – and so that this can be done again and again, any time it is politically exigent to do so, or to suit industry needs.
So they’ll keep testing. The small town of Bolinas, California, north of San Francisco plans to test all 1,600 of its residents, an initiative spawned by a venture capitalist and a pharmaceutical executive.
More book cooking to rescue the #plandemic narrative
In the meantime, the CDC has appeared to employ more book cooking to manufacture the massive outbreak their COVID dud is not delivering.
As reported by WebMD on April 18, the CDC offers another report, not a study, done by some East Coast research assistants, which “repurposes” “CDC data of cases of influenza-like-illness, or ILI,” to estimate that at least 8.7 million people were infected with “coronavirus” (SARS-CoV-2) across the US during a three-week period they studied in March. Although WebMD says the authors revised their estimate down from 28 million, the non-peer-reviewed report still stands in its original form, asserting that only 1 out of every 100 cases was detected in the US during the period studied (March 8 – 28):
“Here, we show how publicly available CDC influenza-like illness (ILI) outpatient surveillance data can be repurposed to estimate the detection rate of symptomatic SARS-CoV-2 infections. We find a surge of non-influenza ILI above the seasonal average and show that this surge is correlated with COVID case counts across states. By quantifying the number of excess ILI patients in March relative to previous years and comparing excess ILI to confirmed COVID case counts, we estimate the syndromic case detection rate of SARS-CoV-2 in the US to be approximately 1 out of 100. This corresponds to at least 28 million presumed symptomatic SARS-CoV-2 patients across the US during the three-week period from March 8 to March 28. Combining excess ILI counts with the date of onset of community transmission in the US [presumed], we also show that the early epidemic in the US was unlikely to be doubling slower than every 3.5 days. Together these results suggest a conceptual model for the COVID epidemic in the US in which rapid spread across the US are [sic] combined with a large population of infected patients with presumably mild-to-moderate clinical symptoms.” (emphasis and interjections ours)
Their research has not been peer reviewed, though the researchers have said their findings coincide with the much-criticized Santa Clara County study. But all they have done here is include “syndromic” reports of flu-like illness to manufacture a population of 28 million ‘undocumented’ cases of “mild to moderate” COVID. That’s a pretty wide definition of “asymptomatic”. We say it’s not a definition of “asymptomatic” at all. But WebMD says this new model proves COVID is “more widespread and less severe.”
Beginning April 3, the CDC also began issuing a “COVID surveillance” report in which they include: “Visits to outpatient providers and emergency departments for illnesses with symptom presentation similar to COVID-19,” mainly “flu-like illness” (ILI) and pneumonia.
In addition, the CDC also updated its clinical criteria and added six new symptoms to its list of COVID symptoms, including: chills, repeated shaking with chills, new loss of taste or smell, muscle pain, headache and sore throat. Taken together with the WHO clinical guidance, which also lists anorexia, malaise, fatigue and nasal congestion, among others as mild symptoms of COVID, there appears to be few symptoms under the sun that would not qualify as a COVID symptom.
Nonetheless, corporate government and its lackeys persist in the idea that they have to hunt down legions of “asymptomatic spreaders” of a disease they have yet to prove exists on the basis of any symptom they decide is a “COVID” symptom.
These are the same people who have trained the public to call totalitarian state lockdowns of healthy people, “quarantines”, which are presumably only for sick people – not the healthy.
Alt media does not seem to understand what it is advancing in its promotion of this ‘less deadly, more widespread’ narrative, which is unfortunately, more pretext for medical surveillance and more lockdowns – not the end of the lockdown – and false justification for the presumed existence of COVID and “novel coronavirus”.
Indeed, in China, “second wave” lockdowns have already been reported.
And, for those who still think this is a US government–created bioweapon, we think this statistical story shows that the government would not have to invent a pandemic if it actually existed.
6 Comments
https://www.armstrongeconomics.com/international-news/disease/youtube-banned-video-of-the-doctors/#.Xqqsr__CPBU.link
https://www.armstrongeconomics.com/international-news/disease/are-ventilators-kill-people-in-new-york-city/#.XqqtDH5pOFE.link
https://www.armstrongeconomics.com/world-news/climate/merkel-reveal-this-is-about-climate-change/#.XqqtX_d580U.link
This one let me thinking…
“As people are now aware that the case and death counts for the alleged COVID-19 disease have been fabricated and inflated in many (and likely most) countries”
Who and how many are those “people”?!
The who and why is wrapped up with a bow on top by this well done piece of investigative journalism. https://youtu.be/1Z5VYqJqrtI
https://www.infowars.com/army-of-medical-brown-shirts-being-created-on-a-national-level/